Internal industry audit data shows that 80% of ABA session notes fail at least one payor requirement. That number changes the conversation. ABA session notes aren't just paperwork. They affect reimbursement, continuity of care, and whether a family can clearly understand what happened in therapy.
As a practitioner, I've seen the same tension over and over. Clinicians need notes that stand up to audits. Parents need notes that make sense in real life. When those goals drift apart, everyone loses. The strongest ABA session notes do both. They document medical necessity with clean, objective data, and they create a usable record that helps families support progress between sessions.
Table of Contents
- Why Most ABA Session Notes Fail and How to Fix Yours
- The Anatomy of a High-Quality ABA Session Note
- From Vague to Valuable How to Write Objectively
- ABA Note Templates and Real-World Examples
- Privacy Storage and Documentation Best Practices
- Turn Notes into Actionable Insights for Your Family
Why Most ABA Session Notes Fail and How to Fix Yours
The problem usually isn't that the therapist did poor work. The problem is that the note doesn't prove what happened in a way a payor can verify. A session may have been productive, responsive, and clinically thoughtful, but if the documentation is vague, incomplete, or missing objective data, it can still fail review.
That's why the 80% failure rate matters so much. It points to a documentation gap, not just an administrative annoyance. When notes miss payor requirements, clinics face delays, denials, and extra rework. Families feel that disruption too, especially when funding interruptions affect scheduling or consistency of care.
What usually goes wrong
In day-to-day practice, weak notes tend to fail for a few predictable reasons:
- They describe impressions instead of observations. “Client was frustrated” is weaker than a direct description of what the client did.
- They skip measurable performance. Without counts, percentages, duration, or trial results, the note doesn't show response to intervention.
- They lose the treatment thread. A good note connects behavior, intervention, and outcome in one clinical story.
- They ignore the family's perspective. A compliant note can still be nearly useless to a parent if it's packed with jargon and no practical meaning.
Good ABA session notes answer three questions fast: What happened, what was done, and what should happen next?
The fix is simpler than people think
The best correction isn't writing longer notes. It's writing cleaner ones. Strong notes use observable language, quantified data, and a structure that makes it easy for another professional to follow the session from start to finish.
That shift helps more than billing. It improves supervision, makes treatment adjustments easier, and gives caregivers a clearer view of progress. When a note says exactly what the child did, what prompt level was needed, and how the intervention affected responding, the care team can act on it.
A useful standard is this: if another BCBA, an auditor, or a parent reads the note, they should be able to understand the session without guessing. If they have to infer what “did well” or “challenging behavior” means, the note isn't finished.
The Anatomy of a High-Quality ABA Session Note
A high-quality ABA session note has two jobs. It must meet clinical and funding requirements, and it must preserve enough detail to guide the next decision. That's why structure matters. A scattered paragraph might capture effort, but it rarely captures a defensible clinical record.
The most reliable format is SOAP. According to Alpaca Health's practical guide for BCBAs, expert-level notes follow the SOAP framework, and the Objective section must quantify behavior using frequency, duration, or percentage of correct responses rather than subjective phrases like “appeared engaged.”

What belongs in each SOAP section
| Section | What it should include | What to avoid |
|---|---|---|
| Subjective | Relevant caregiver report, changes in sleep, routines, illness, medication, or transitions that may affect the session | Guessing or treating caregiver report as measured fact |
| Objective | Observable behavior, trial counts, frequency, duration, prompt levels, goal-linked performance | Emotional labels, broad judgments, unsupported conclusions |
| Assessment | Clinical interpretation of the data, comparison to prior performance, response to intervention | Repeating raw data with no analysis |
| Plan | Specific next steps, what will continue, change, fade, or be monitored next session | Generic statements like “continue treatment” with no detail |
The non-negotiable details
Even strong clinical writing can fail if the administrative basics are sloppy. Every note should clearly include the client's identifying information, session date, start and end time, duration, location, provider identity, and signature requirements used by the organization.
Those details look simple, but they're often the first things auditors notice. Missing timestamps or missing identifiers can undermine an otherwise solid note because they create doubt about whether the record is complete and attributable.
Practical rule: If a required field appears on your note template, treat it as clinical content, not clerical filler.
What makes a note clinically useful
The difference between an acceptable note and a strong one is linkage. A strong note doesn't just list behaviors and interventions separately. It connects them.
For example, if the client engaged in task refusal, the note should show what the refusal looked like, when it happened, what intervention was used, and how the response changed. That creates a treatment narrative grounded in data. It also makes supervision more efficient because the BCBA can evaluate treatment integrity and decision-making from the record.
Teams that want a cleaner workflow often benefit from reviewing their note structure alongside a dedicated special education data collection workflow so the data gathered during sessions matches what the note will later require. When collection and documentation line up, note-writing gets faster and more accurate.
From Vague to Valuable How to Write Objectively
Most weak ABA session notes fail in the same place. They use words that sound informative but don't describe behavior. “Upset,” “uncooperative,” “good session,” and “tried hard” may feel natural in conversation, but they don't hold up clinically.
That's not a minor style issue. According to Motivity's discussion of ABA session note pitfalls, vague language and omitted context appear in 35% of non-compliant notes, and failure to include a clear Plan for Next Session appears in 40% of rejected logs.
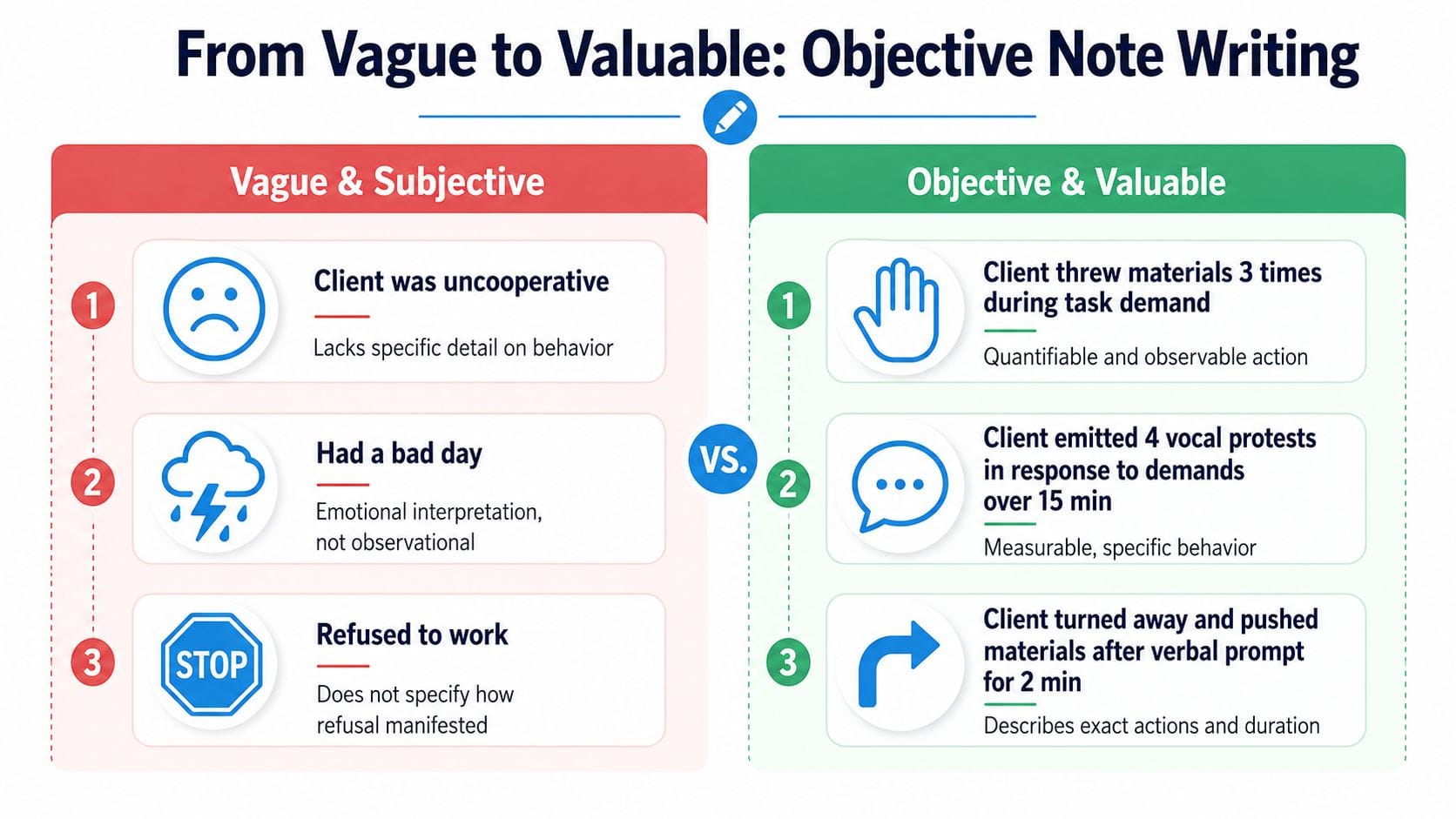
What objective writing sounds like
Here's a simple comparison that clinicians and parents can both use.
| Weak wording | Better wording |
|---|---|
| Client had a bad day | Client engaged in vocal protest during work demands and required repeated redirection before returning to task |
| Client was uncooperative | Client turned away from materials, pushed task items aside, and did not respond to the initial instruction |
| Client did well with communication | Client independently requested preferred items across multiple opportunities with fewer prompts than in the prior session |
| Session was challenging | Session included interruptions related to refusal behavior and reduced task engagement during transitions |
The stronger version doesn't need inflated language. It needs observable action.
Replace interpretation with observation
A quick rule for writing objective notes is to ask, “Could a camera verify this?” If the answer is yes, it probably belongs in the note. If the statement depends on mind-reading or emotional interpretation, rewrite it.
Use this pattern:
- Describe the antecedent. What happened right before the behavior?
- Describe the behavior. What did the client do?
- Describe the consequence or intervention. What response followed, and what changed?
That approach is especially important when documenting aggression, elopement, refusal, repetitive behavior, or communication attempts. Clear operational descriptions protect the therapist, help the supervisor, and make the record more understandable for caregivers.
Context matters more than many notes show
Objective writing isn't only about counting behavior. It also means documenting barriers and environmental factors that changed session performance. Noise, schedule changes, illness, transitions, staffing changes, unfamiliar settings, and caregiver report can all matter when interpreting data.
If behavior changed, the note should help the next reader understand why that change may have happened.
A bare summary can miss the entire clinical point. “Client completed fewer programs today” tells almost nothing. A more useful note might reflect that the session started late after a difficult transition, or that caregiver reported disrupted sleep, or that the environment changed.
A better ending improves the whole note
Many notes lose strength at the end. They document the session but fail to state the next clinical step. The Plan should answer what the team will do with the information just collected.
A useful plan might indicate that a prompting strategy will continue, a target will be faded, a behavior reduction procedure will be modified, or caregiver coaching will focus on a specific routine. The plan doesn't need to be long. It does need to be actionable.
ABA Note Templates and Real-World Examples
Templates help because they reduce decision fatigue. When the framework is already built, the therapist can focus on accuracy instead of formatting. That matters in busy clinics, in-home sessions, and supervision workflows where time gets tight fast.
A strong template should support the SOAP format and prompt the writer to include quantified performance tied to treatment goals. That aligns with the expectations used for billing codes such as 97153, 97155, and 97156, where the Objective section needs measurable data to support medical necessity, as described in this ABA session note guide.
A simple SOAP note example
Subjective
Caregiver reported a difficult morning transition and lower than usual interest in breakfast. No medication changes were reported. Client arrived willing to enter the work area with one prompt.
Objective
Client participated in skill acquisition targets involving listener responding, requesting, and transition tolerance. During non-preferred table tasks, client engaged in vocal protest and pushed materials away following instructional demands. Therapist used reinforcement, visual supports, and prompt fading. Client showed stronger responding during preferred-item requesting than during transition tasks.
Assessment
Performance suggests that motivation was higher during communication targets than during demand-heavy tasks. Refusal behavior appeared most likely during transitions into structured work and decreased after reinforcement and clearer task sequencing were introduced.
Plan
Continue current communication goals. Modify transition supports next session by front-loading the visual schedule and reducing delay between instruction and reinforcement. Monitor refusal during work initiation and review caregiver strategies for morning transitions.
A parent-friendly ABC example
Parents don't always need a full clinical SOAP note at home. Often, a brief ABC log captures what matters most.
- Antecedent: Asked to stop tablet and come to the table
- Behavior: Turned away, yelled, pushed chair back
- Consequence: Parent paused demand, gave visual reminder, child came to table after a short break
That kind of entry is useful because it captures trigger, response, and outcome without requiring clinical jargon. It also creates a cleaner record for therapists who are trying to identify patterns across settings.
For teams refining spoken observation into written documentation, some principles from voice-capture lab note best practices are surprisingly relevant. The key overlap is simple: capture observations close to the event, keep descriptions concrete, and convert spoken shorthand into structured records before memory blurs the details.
What a template should prompt every time
Not every organization uses the same form, but the strongest ABA session note templates usually force the writer to answer these questions:
- What goals were addressed
- What behavior was observed
- What intervention was used
- What data showed the client's response
- What should change next
Here's a quick visual example of how clinicians think through note structure in practice:
A template is doing its job when it improves consistency without turning the note into a script. Families benefit from that too. When the structure is consistent, they can track what changed from one session to the next without decoding a different writing style every day.
Privacy Storage and Documentation Best Practices
A strong note that's late, unsecured, or impossible to retrieve creates a different kind of risk. Good documentation practice isn't only about wording. It's also about timing, storage, and safe sharing.
According to BACB-cited industry standards summarized here, ABA session documentation must be securely stored for at least 7 years and completed within a 24 to 72 hour window after the session. Those two requirements shape the entire workflow.
Why timing matters
Clinically, prompt documentation protects accuracy. The longer a therapist waits, the more likely the record drifts toward summary instead of detail. Small but important facts get lost first. Prompt level, environmental changes, exact topography, and caregiver-reported context are often the first casualties of delay.
From a compliance standpoint, late notes also raise questions about reliability. If the note doesn't reflect the session close to when it occurred, it becomes harder to defend as a precise treatment record.
Write close enough to the session that you still remember what the client did, not just how the session felt.
What secure storage actually means in practice
Secure storage means more than “saved somewhere.” Teams need a system that protects confidentiality, limits unnecessary access, and makes records retrievable when a payer, supervisor, or authorized caregiver needs them.
A workable standard usually includes:
- Access control: Only people involved in treatment or authorized review should see the record.
- Consistent naming and filing: Notes should be easy to find by client, date, and service type.
- Protected sharing: If information is shared with schools, physicians, or caregivers, it should be sent through approved channels.
- Retention discipline: Records shouldn't disappear because a staff device changes or a family is discharged.
Families also benefit from using an organized record system for evaluations, insurance paperwork, and therapy documentation. A practical starting point is this guide on how to organize autism records for evaluations, which mirrors the same logic clinicians rely on when building audit-ready files.
Privacy is part of trust
Parents are far more likely to engage with documentation when they trust how it's handled. That trust grows when providers explain who can access notes, how long they're kept, and how session summaries are shared.
Privacy and usefulness don't compete with each other. When the documentation system is secure and organized, everyone can spend less time hunting for records and more time using them well.
Turn Notes into Actionable Insights for Your Family
Families often receive ABA session notes that satisfy a payer but don't help much at home. That disconnect is common. Research summarized here reports that 78% of parents feel disconnected from ABA progress because notes are jargon-heavy, and it also notes that integrated tracking across sleep, diet, and behavior can improve intervention accuracy by 43% in systems that support that kind of analysis, which traditional note formats often don't (Passage Health).
That gap matters because children don't live in isolated treatment blocks. A rough night of sleep, a shift in appetite, a medication change, a school transition, or a new routine can affect the entire day. If those variables live in separate notebooks, texts, and memory, the pattern is easy to miss.

What families should pull from session notes
A parent doesn't need every billing detail. They usually need a short list of practical answers:
- What improved: Which skill or routine was stronger today?
- What was hard: Which trigger, transition, or demand led to difficulty?
- What helped: What response from the therapist reduced the problem or supported success?
- What to try at home: What should the family continue, prompt, avoid, or monitor?
When therapists write notes with that translation in mind, families are more likely to follow through. The note becomes a tool for continuity instead of a document that gets filed and forgotten.
Look for patterns across domains
The most useful insights often appear when session records are compared against daily life data. A rise in refusal behavior may line up with poor sleep. Increased dysregulation might coincide with a disrupted routine or a missed meal. Better communication might cluster around stronger morning regulation.
That kind of pattern detection is hard to do with scattered records. It gets easier when families keep consistent logs that can be reviewed alongside therapy notes. Even general retention habits matter here. For parents trying to build sustainable record systems, broader resources like this Typist guide to file retention can help frame how to keep important documents organized over time without creating digital chaos.
The most helpful note is the one that changes what the family does next.
A more usable standard for progress tracking
Clinicians need objective documentation. Families need clarity they can use on Tuesday afternoon when a routine falls apart. Those needs can live in the same system if the data is structured well and reviewed consistently.
Parents who want a cleaner way to see progress over time can start with a practical framework for how to track autism therapy progress. The core idea is simple. Track the behaviors, routines, and contextual factors that shape your child's day, then review them in one place often enough to spot changes while they still matter.
ABA session notes are most valuable when they stop being the end of documentation and start becoming the beginning of insight.
Guiding Growth helps families turn scattered therapy notes, behavior logs, sleep patterns, food observations, medications, and daily routines into one organized picture. If you want a simpler way to log what's happening, reduce guesswork, and collaborate with your child's care team, explore Guiding Growth.


