Some of the hardest moments as a parent happen when your child's behavior seems to point in two directions at once. Your child might spend a long time absorbed in a favorite activity, then seem unable to follow a simple routine. They might care a great deal about other people, yet still miss social cues in a group. You're left wondering whether this looks more like ADHD, autism, or something that doesn't fit neatly into either box.
That confusion is common. It doesn't mean you're overthinking, and it doesn't mean your child is being inconsistent on purpose. It usually means the behavior needs context. The same outward action, such as not responding, refusing a transition, or interrupting, can come from very different underlying reasons.
This guide is for parents who want clearer language, better observation, and a more grounded way to talk with professionals. If you're also trying to prepare for next steps, this overview of what to expect during an autism evaluation can help you feel less blindsided by the assessment process.
Table of Contents
- Is It ADHD or Autism or Both
- Core Differences Between ADHD and Autism
- Untangling Overlapping Traits in Daily Life
- How Signs of ADHD and Autism Evolve with Age
- Understanding Co-Occurrence The Reality of AuDHD
- Preparing for an Assessment What to Track and Tell Clinicians
- Immediate Strategies to Support Your Child Today
Is It ADHD or Autism or Both
A parent might say, “My child can focus for hours on one thing, so how could this be attention trouble?” Another might say, “My child wants friends, so how could this be autism?” Those questions make sense. They're also where many families get stuck.
ADHD and autism can look similar from the outside. A child may seem distracted, emotionally overwhelmed, socially awkward, rigid, impulsive, or inconsistent. What matters is not only what the behavior looks like, but why it happens.
Take a morning routine. One child may bounce from socks to breakfast to a toy on the floor because every new stimulus pulls their attention away. Another child may get stuck because the shirt feels wrong, the order changed, or they can't shift mentally from one step to the next. Both children may end up late and upset. The path there is different.
A behavior is easier to understand when you ask, “What made this hard for my child in this moment?”
Parents also get confused because children aren't textbook examples. A child with ADHD may have real social trouble. An autistic child may be affectionate, funny, chatty, and eager to connect. Some children show traits of both, which can make the overall pattern feel contradictory.
If your child seems to crave structure but can't carry it out, or seeks connection but struggles to manage it, you're not failing to “figure it out.” You may be seeing a more complex neurodevelopmental profile that deserves careful observation rather than quick assumptions.
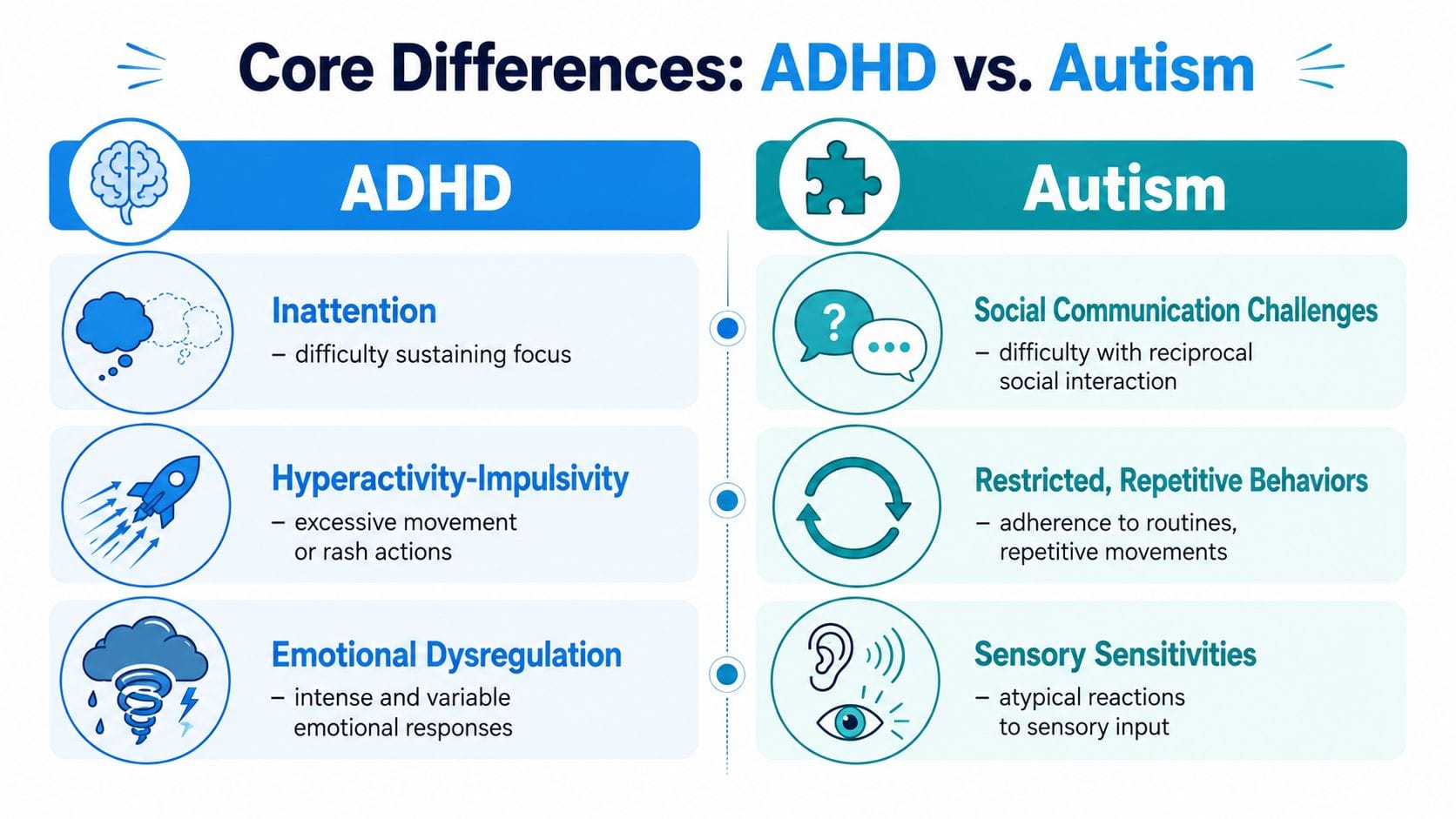
Core Differences Between ADHD and Autism
At the broadest level, ADHD is mainly about regulation of attention, activity level, and impulsive behavior. Autism is mainly about social-communication differences plus restricted or repetitive patterns, including a stronger pull toward sameness and routine. A concise overview from Autistica's guide to ADHD and autism also notes that people with ADHD are more likely to seek novelty, while autistic people are more likely to prefer routine and structure.
A quick side by side view
| Characteristic | ADHD (Attention-Deficit/Hyperactivity Disorder) | Autism Spectrum Disorder (ASD) |
|---|---|---|
| Core pattern | Difficulty regulating attention, activity, and impulse control | Social-communication differences and restricted or repetitive behaviors |
| Attention style | Attention may shift quickly, especially when tasks are boring or unrewarding | Attention may become very narrow or hard to shift, especially around preferred interests or routines |
| Relationship with routine | May resist routine because of boredom, forgetfulness, or poor follow-through | Often finds comfort in predictability, sameness, and structure |
| Social presentation | Usually wants connection but may interrupt, miss timing, or act impulsively | Social communication may look qualitatively different, including how cues are read and responded to |
| Change and transitions | May move too fast into new things | May struggle to disengage from the current activity or cope with change |
| Common parent impression | “My child knows what to do but can't stay with it” | “My child wants things to feel consistent and gets thrown off when they don't” |
ADHD is also more common overall. The CDC estimate cited by Autistica says 11.4% of U.S. children ages 3 to 17 had ever been diagnosed with ADHD in 2022, while autism prevalence is described there as about 1 in 31 U.S. children and around 1% to 2% globally in broader clinical estimates included in that same overview.
Why parents often mix them up
The confusion starts when real life doesn't separate traits neatly. A child who talks over others may be impulsive. A child who doesn't answer a question may be overloaded, focused elsewhere, unsure how to respond, or still processing language. Outwardly, both can look like “not listening.”
If your child's profile also overlaps with learning or processing differences, it can help to read about related patterns such as nonverbal learning disorder vs autism. Sometimes what seems like one issue is several interacting pieces.
Some families are also weighing multiple possibilities at once. If worry, restlessness, or shutdowns are muddying the picture, this guide on the difference between ADHD and anxiety can help you think more carefully about what's driving the behavior you're seeing.
Big picture: ADHD is usually centered on regulation. Autism is usually centered on social communication, repetitive patterns, and sameness. The overlap happens in day to day behavior, not in the core definition.
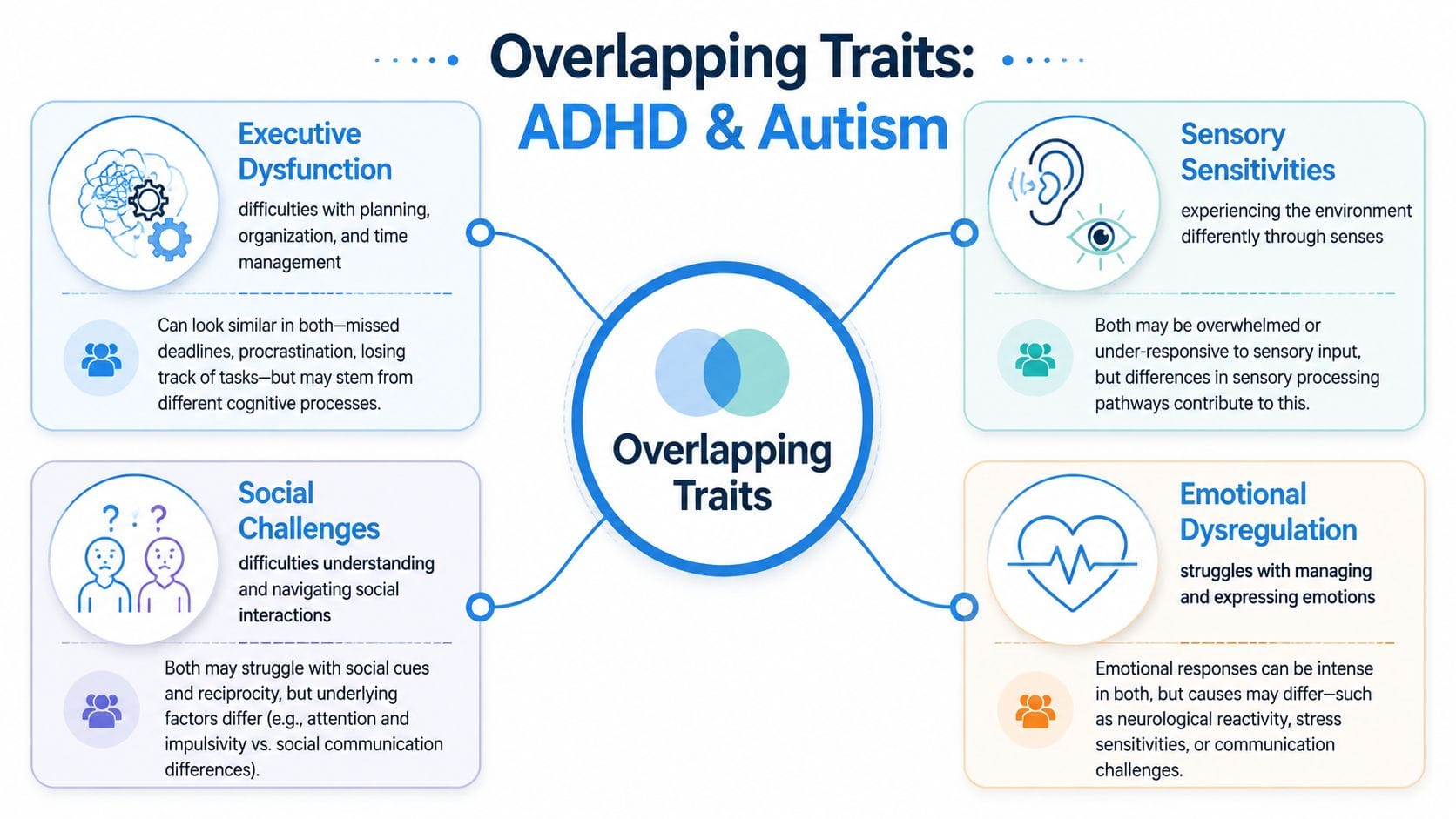
Untangling Overlapping Traits in Daily Life
Many parents don't struggle with the labels. They struggle with the overlap. Their child has trouble starting tasks, melts down during transitions, misses social cues, and seems flooded by daily life. That can happen in ADHD, autism, or both.
A 2024 review in Frontiers in Psychiatry found that both conditions involve executive function difficulties, but the pattern isn't the same. ADHD is more strongly linked to problems with inhibition and sustained attention, while autism is more associated with cognitive flexibility difficulties. The review also notes that executive function impairment is generally worse in ADHD overall, while children with both ADHD and ASD may show the heaviest combined burden.
When inattention is not the same thing
“Inattention” sounds simple, but it isn't. One child may look away because every nearby sound, movement, or thought steals their focus. Another may ignore you because they are locked onto one mental track and can't shift out of it easily.
That distinction matters. If a child can focus intensely on a preferred activity but struggles to disengage, the pattern may fit autism-related attentional style more than classic ADHD distractibility. A clinical review in this NIH-hosted paper on ADHD and ASD differentiation noted that attentional symptoms in autism can look like “not listening” or difficulty shifting focus, rather than the short attention span and excessive distractibility more typical of ADHD. That review also reported selective attention in 98% of ASD children compared with 21% in ADHD-I/Combined groups.
If your child can stay with one preferred task for a very long time, don't assume that rules out attention difficulty. It may mean the attention problem is about shifting, not sustaining.
Social struggles can come from different places
A child with ADHD may interrupt because the thought feels urgent and impulse control breaks down. They may dominate a game, miss turn-taking, or talk too much because regulation is hard in the moment.
An autistic child may want connection but struggle with the hidden rules of conversation. They may miss facial cues, interpret language at face value, or not know when to enter a group interaction. The social challenge is less about acting too fast and more about processing and reciprocity.
Here are two examples that look similar but mean different things:
- Not joining a group game: One child may drift away because the game isn't stimulating enough. Another may want to join but not know how to break into the social flow.
- Talking at length: One child may blurt and jump topics rapidly. Another may speak in depth about a focused interest without noticing the listener's cues.
- Seeming rude: One child may act before thinking. Another may not realize a response sounds blunt.
The hidden why behind daily friction
Sensory differences and emotional dysregulation can also blur the lines. A child may explode in a grocery store because of noise, lights, hunger, waiting, frustration, or all of them at once. The useful question is not “Was that ADHD or autism?” The useful question is “What load was too high for my child in that setting?”
If you want better answers, track what happened before, during, and after hard moments. A guide on how to track and understand behavioral triggers can help you move past vague notes like “bad day” and toward patterns that are actually useful.
Practical rule: Don't log only the behavior. Log the demand, the setting, the sensory load, the transition, and what helped recovery.
How Signs of ADHD and Autism Evolve with Age
Traits don't stand still. They change as a child's environment changes and as expectations rise. A behavior that seemed minor in preschool can become much more visible when school, friendships, homework, and independence all demand more regulation.
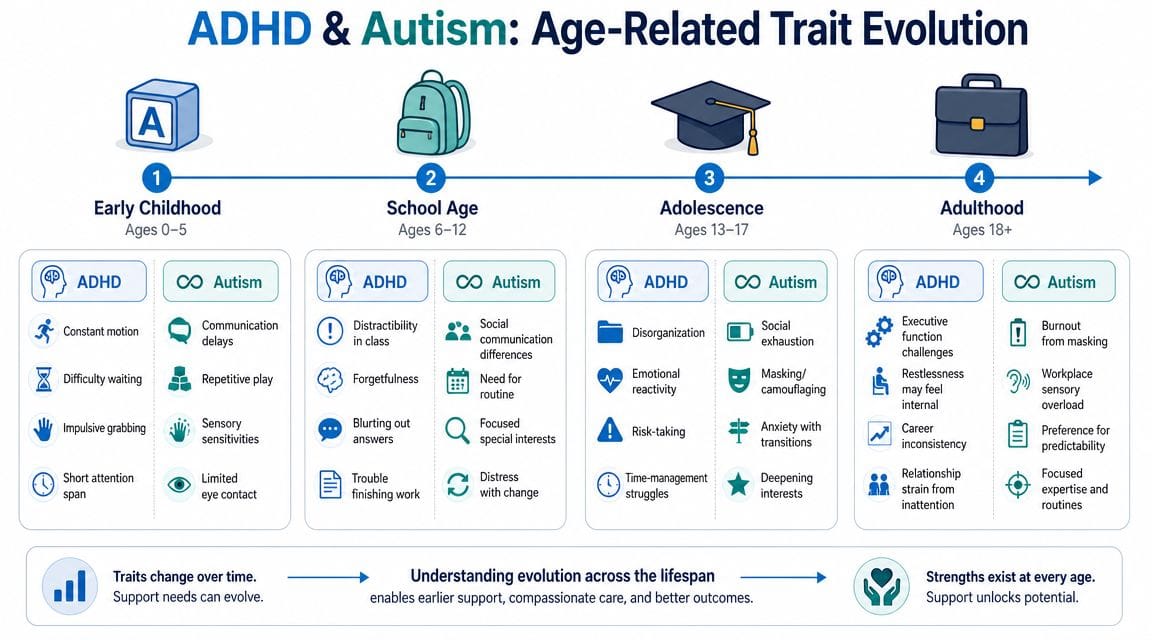
Early childhood
In toddlers and preschoolers, ADHD may show up as constant motion, short bursts of engagement, climbing, grabbing, bolting, or struggling to wait. The child often seems driven toward action and novelty.
Autism may show up earlier through social-communication differences, repetitive play, strong sensory reactions, or distress around change. A child may line up toys, repeat actions, or become very upset if a routine shifts unexpectedly.
A useful distinction is this. ADHD often looks like moving away from structure. Autism often looks like needing structure and feeling unsettled without it.
School age years
Once school begins, demands become less forgiving. Children are asked to sit, shift, listen in groups, manage materials, read social cues, and handle a crowded sensory environment. This is often when adhd and autism differences become more noticeable.
In ADHD, teachers may notice unfinished work, blurting, distractibility, and inconsistent performance. The child may understand the material but struggle to organize, start, or complete the task.
In autism, school challenges may center more on hidden social rules, sensory strain, inflexible thinking, or intense stress during transitions. Some children hold it together all day and then fall apart at home because the effort of coping has built up.
A child who looks “fine” at school but collapses after school isn't necessarily overreacting. They may be reaching the end of what their nervous system can manage.
Adolescence
Teen years bring social complexity, heavier workloads, and more pressure to self-manage. For some young people with ADHD, this is when disorganization, time blindness, emotional reactivity, and impulsive decision-making become more costly.
For autistic teens, adolescence can increase social exhaustion and the pressure to mask differences. Some become more anxious, shut down more often, or seem increasingly withdrawn because the social world now requires rapid interpretation and constant self-monitoring.
In both groups, strengths may also become clearer. A teen may show creativity, humor, loyalty, deep knowledge, or unusual persistence. The challenge is making sure support grows with the child, instead of assuming age alone will smooth things out.
Understanding Co-Occurrence The Reality of AuDHD
Some children don't fit cleanly into one category because they meet criteria for both. That combined profile is often called AuDHD. For many families, hearing this is a relief. It explains why their child can seem pulled in opposite directions.
Why this recognition came later
For years, the diagnostic system itself got in the way. Children's Hospital of Philadelphia summarized research on ADHD in autistic adults and noted that the DSM did not allow simultaneous autism and ADHD diagnoses until DSM-5 in 2013. That change matters because it opened the door to more accurate identification instead of forcing clinicians to choose one or the other.
That same summary reported that in a large population-based study of more than 3.5 million adults, 27% of autistic adults without intellectual disability had co-occurring ADHD, which was about a 10-fold increase over the general Medicaid-enrolled population. Among autistic adults with intellectual disability, the rate was 40%. Broader reviews cited there also place ADHD prevalence among people with ASD often in the 50% to 70% range.
What AuDHD can look like at home
A child with AuDHD may want routine and also resist starting it. They may crave sameness and also seek stimulation. They may have deep interests, poor follow-through, intense focus, and difficulty shifting.
Parents sometimes think this means the child is inconsistent or oppositional. It usually means both neurodevelopmental profiles are active at the same time.
You don't have to pick one explanation if your child's behavior clearly points to both. Combined profiles are real, and support works better when it reflects that reality.
Preparing for an Assessment What to Track and Tell Clinicians
When families prepare for an assessment, they often bring a general story. “He struggles with focus.” “She has meltdowns.” “School says he doesn't listen.” That's understandable, but clinicians need a more detailed picture.
Track patterns not isolated moments
The most helpful notes show patterns across settings. A clinician is trying to understand whether the main issue is attention regulation, social communication, cognitive flexibility, sensory load, or some combination of these.
One practical distinction comes from the earlier NIH-linked clinical review. If a child can sustain intense focus on preferred tasks but struggles to disengage, that pattern is more consistent with an autism-related attentional style than classic ADHD distractibility. That means your notes should capture not just “focus problems,” but what kind of focus problem you're seeing.
Instead of writing “didn't listen,” write down what happened:
- What was the demand: Multi-step direction, conversation, homework, cleanup, transition.
- What was happening around them: Noise, siblings, hunger, fatigue, crowded room, unfamiliar place.
- How your child responded: Ignored, delayed, argued, melted down, got stuck, wandered off.
- What changed the outcome: Repetition, visual cue, reduced noise, first-then language, break, movement.
What details help clinicians most
The strongest observations are concrete and time-linked. They don't need to be polished. They need to be specific.
A useful record often includes:
- Attention pattern: Does your child get distracted by everything around them, or do they get stuck and can't shift away from what they're already doing?
- Social pattern: Are problems mostly about impulsive behavior in conversation, or about reading cues, reciprocity, and joining in?
- Transition pattern: Is the struggle about boredom and low motivation, or distress when plans change?
- Sensory load: Which settings tend to precede shutdowns, meltdowns, refusal, or escape behavior?
- Recovery style: What helps your child settle. Quiet space, movement, alone time, deep pressure, snack, clear instructions, or reduced demands.
If you want a more detailed picture of how formal evaluation often works, this overview of understanding childhood ADHD assessments is a useful companion read for parents who want to know what clinicians may ask and observe.
You can also ask teachers, grandparents, and therapists for examples rather than impressions. “He's impulsive” is less helpful than “He calls out answers before the question is finished and gets upset when redirected.” “She's socially withdrawn” is less helpful than “She stays near peers but doesn't know how to enter play unless an adult scripts it.”
Bring examples from home, school, and community settings. A child's profile often looks different depending on the demands of the environment.
Immediate Strategies to Support Your Child Today
You don't need a final diagnosis to start making life easier. Good support is often practical, low-pressure, and responsive to what your child's nervous system handles best.
Reduce friction in the environment
Start with predictability. Many children with ADHD, autism, or both do better when the environment carries some of the load for them.
Try a few supports and watch what changes:
- Use visual routines: A simple morning checklist with pictures or short words can reduce repeated verbal prompts.
- Externalize time: Visual timers often work better than frequent reminders because they make time visible.
- Create a recovery space: A calm corner with preferred sensory supports can help after school, during transitions, or after overload.
- Lower transition shock: Give a warning before stopping a preferred activity, then pair it with a concrete next step.
Shorter instructions also help. One direction at a time is often easier to process than a long chain of spoken information.
Make communication easier to process
Children usually do better when adults say less, mean exactly what they say, and avoid abstract language in high-stress moments. “Shoes on, then car” is easier to use than “Come on, we're running late and you know what you should be doing.”
You can also adjust how you respond to hard moments:
- Pause before correcting. Ask yourself whether the behavior came from skill difficulty, overload, or true defiance.
- Describe what you see. “You're stuck” or “That change felt hard” often lands better than “Why are you doing this?”
- Solve one problem at a time. If your child is overwhelmed, don't add a lecture on tone, manners, and responsibility all at once.
Support works best when it targets the reason behind the behavior, not just the behavior itself.
Even simple experiments can teach you a lot. If headphones reduce distress in noisy places, that tells you something. If a visual checklist cuts down morning conflict, that tells you something too. Keep what helps, drop what doesn't, and stay curious about patterns rather than chasing perfect behavior.
If you want one place to organize those patterns, Guiding Growth can help. It gives parents a practical way to log behavior, sleep, diet, routines, medications, appointments, and contextual triggers without relying on scattered notes. Over time, those entries can make it much easier to spot what's driving hard moments, what supports are helping, and what details to bring into conversations with teachers, therapists, and clinicians.
Authored using Outrank


