You've probably landed here after typing autism adhd test into a search bar late at night, with a dozen tabs open and a knot in your stomach.
Maybe your child can talk for an hour about one favorite topic but seems to miss directions at school. Maybe they melt down after a change in routine, avoid noisy places, struggle to sit still, or seem socially unsure one day and intensely chatty the next. Parents often tell me the hardest part isn't one behavior. It's the mix of behaviors that doesn't fit neatly into a single box.
That confusion makes sense. Autism and ADHD can overlap in ways that are hard to sort out from everyday observation alone. And when you're the person living with those patterns every day, it can be even harder to know what's meaningful, what's age-typical, and what needs a closer look.
The good news is that you do not need to figure this out alone. There is a real process for getting answers, and it's much more thoughtful than a quick online quiz. The most helpful thing you can do right now is learn how that process works, what different tools measure, and how your own observations can help a clinician understand your child clearly.
Table of Contents
- Your Child's Behavior is Complex and You Need Answers
- Screening vs Diagnosis The First Important Distinction
- Common Screening Tools You Might Encounter
- A Closer Look at Formal Diagnostic Instruments
- Interpreting Results and Understanding Spiky Profiles
- Your Next Steps After an Evaluation
- Prepare for an Assessment with Guiding Growth
Your Child's Behavior is Complex and You Need Answers
You notice one child who chats comfortably at home but goes quiet and overwhelmed at school. Another child cannot sit through dinner, yet can spend an hour arranging toys in the same pattern or talking about one favorite topic in remarkable detail. A parent looking at those patterns is often trying to answer a hard question. Are these signs of ADHD, autism, both, or a different developmental difference altogether?
That uncertainty can feel heavy.
It also makes sense. Children do not read like simple checklists. The same child can look flexible in one setting and rigid in another, social with familiar people and shut down with peers, distracted during homework and intensely focused on a preferred activity. What looks inconsistent on the surface often becomes more understandable once someone tracks when behaviors happen, what happened right before them, and how often the pattern shows up across home, school, and community settings.
Parents usually reach this point after hearing several partial explanations. A teacher may notice attention problems. A grandparent may see anxiety or sensory sensitivity. A pediatrician may suggest taking a closer look. School staff may describe one picture, while a medical provider sees another, which is why it helps to understand the difference between school and medical autism evaluations and their legal implications.
The search for an autism adhd test often starts because the picture is mixed.
That is also why parent observation matters so much. A clinician may meet your child for one appointment or a few hours of testing. You see the Monday-morning transitions, the after-school meltdowns, the bedtime routines, the birthday parties, the grocery store trips, and the way your child recovers after stress. Your notes are not extra information. They are part of the foundation of an accurate evaluation.
A useful way to picture the process is to compare it to putting together a puzzle with pieces gathered from different places. The clinician brings training. Teachers bring school-based observations. Your child brings their own profile of strengths and struggles. You bring the longest view of development over time. Tools such as Guiding Growth can help you collect those observations in a structured way, so patterns are easier to spot and easier to share clearly with the professionals involved.
Some families also look into telehealth diagnostic evaluations while they consider assessment options. That can widen access, especially when local services are limited, but the quality of the process still depends on detailed history, behavior patterns across settings, and organized input from the adults who know the child best.
Screening vs Diagnosis The First Important Distinction
Many parents use the phrase autism adhd test to mean any questionnaire, checklist, office visit, or formal evaluation. Clinicians don't use those words interchangeably, and that difference matters.
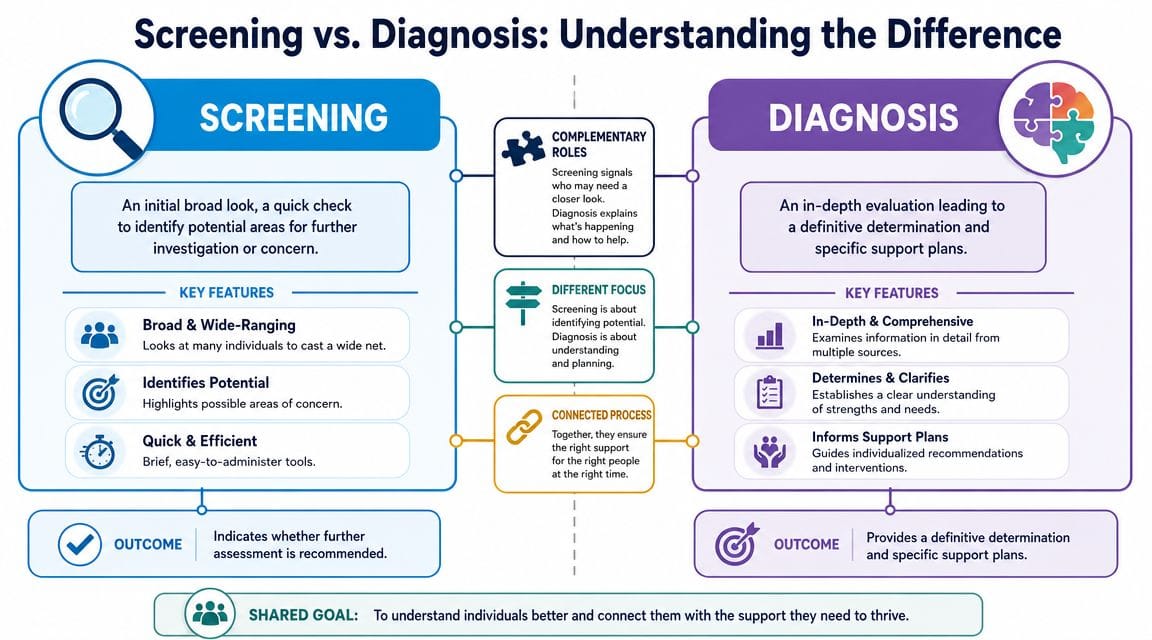
A screening is a quick first look. A diagnosis is a full investigation.
Think smoke alarm versus fire investigation
A screening works like a smoke alarm. It tells you there may be something important to check. It does not tell you exactly what's happening, why it's happening, or what the full picture looks like.
A diagnosis is closer to a full fire investigation. The clinician looks at the pattern, the history, the settings where behaviors show up, and whether those behaviors fit the actual diagnostic criteria.
What a diagnosis really involves
A formal diagnosis is not a single score, scan, or computer task. The clinical literature is clear that there are no standalone biomarkers, cognitive tests, or neuroimaging scans with enough specificity to diagnose ADHD or autism alone. Proper assessment relies on detailed clinical interviews, developmental history, and collateral information from multiple settings, as outlined in this clinical review of adult ADHD and autism assessment.
That means a clinician usually wants more than a symptom checklist. They may ask about:
- Early development such as speech, play, social connection, and sensory patterns
- Current functioning at home, school, and in the community
- Impact on learning, friendships, routines, emotional regulation, and daily life
- Patterns over time rather than one unusually good or unusually hard day
Why a positive screener is not a final answer
Parents often worry when a screener comes back “high risk” or “heightened.” Those results matter, but they don't equal a diagnosis. They mean your child's profile deserves a closer look.
That's especially important when autism and ADHD traits overlap. Inattention can reflect classic ADHD, but it can also appear when a child is overwhelmed by noise, confused by social demands, stuck on a specific interest, or struggling with sensory regulation. A diagnosis sorts out the reason, not just the visible behavior.
Practical rule: If a result gives you a label without asking about development, daily functioning, and behavior across settings, it's not the whole answer.
This is also where school and medical evaluations start to diverge. If you're trying to understand who evaluates what, school vs medical autism evaluations and their legal implications can help clarify the difference between educational eligibility and clinical diagnosis.
Common Screening Tools You Might Encounter
You answer a few questions on a form, add up the score, and hope it will finally tell you what is going on. Many parents arrive at this point tired, worried, and ready for certainty. Screening tools can help, but their real job is narrower. They point toward patterns that deserve a closer look.
That is why your observations matter so much. A screener is a snapshot. Your notes about what happens before, during, and after a hard moment are more like a short video. Clinicians can do far more with that kind of detail.
Autism screeners you may see first
For toddlers, clinicians often start with the M-CHAT-R, a parent questionnaire used in early autism screening. For older teens and adults, you may hear about the Autism Spectrum Quotient (AQ), a self-report measure that looks at autistic traits.
These tools are useful because they are quick and structured. They give families and clinicians a shared starting point. They also have limits. A child who struggles with language, sensory overload, anxiety, or attention may trigger concerns on a screener without the form explaining why those behaviors happen.
That gap matters. Two children can get similar screening results for very different reasons.
If you want a clearer picture before an appointment, a DSM-5 autism checklist for parents can help you organize what you have seen at home, not just your gut feeling in the moment. Many parents also use Guiding Growth to log recurring patterns across settings, which gives the evaluator something more useful than a memory of a stressful week.
Why screening results can feel inconsistent
A screener may suggest concern even when your child seemed fine during a short office visit. The reverse can happen too. That does not mean anyone answered incorrectly.
Children do not show their traits in the same way in every setting. Some hold themselves together at school and fall apart at home. Some copy peers so well that social strain is easy to miss. Others look inattentive when they are overloaded by noise, confused by language, or locked onto one interest.
Adult self-screens can be tricky for similar reasons. People who have spent years masking often describe their inner effort very differently from what others notice. Prosper Health's overview of autism testing for adults explains why self-tests can miss that complexity.
What a clinician is really doing with a screener
A screener works like a smoke alarm. It tells you where to check more carefully. It does not tell you what started the smoke.
So a clinician listens for the story underneath the answer:
Parent report: “He ignores us when we call his name.”
What the clinician wonders: Is he distracted, intensely focused, overwhelmed, or having trouble processing language?Teacher report: “She drifts off and misses directions.”
What the clinician wonders: Does it happen across all tasks, or mostly in noisy, socially demanding, or unstructured parts of the day?Caregiver concern: “Changes in routine lead to huge reactions.”
What the clinician wonders: Is the main driver sensory regulation, anxiety, executive function difficulty, or a mix?
Some evaluations also include cognitive testing, such as the Wechsler Intelligence Scale for Children, because learning profile, language demands, and processing style can shape how screening answers look on paper.
One score rarely captures the whole child. A parent who brings organized observations about patterns over time gives the clinician a much better starting point. That partnership often matters more than any single screener result.
A Closer Look at Formal Diagnostic Instruments
Once concerns move beyond screening, families enter a more detailed part of the process. These are the tools people often mean when they ask about an autism adhd test, but even here, no single instrument stands alone.
To understand the autism side, it helps to see two of the better-known tools side by side.
Autism tools focus on observation and history
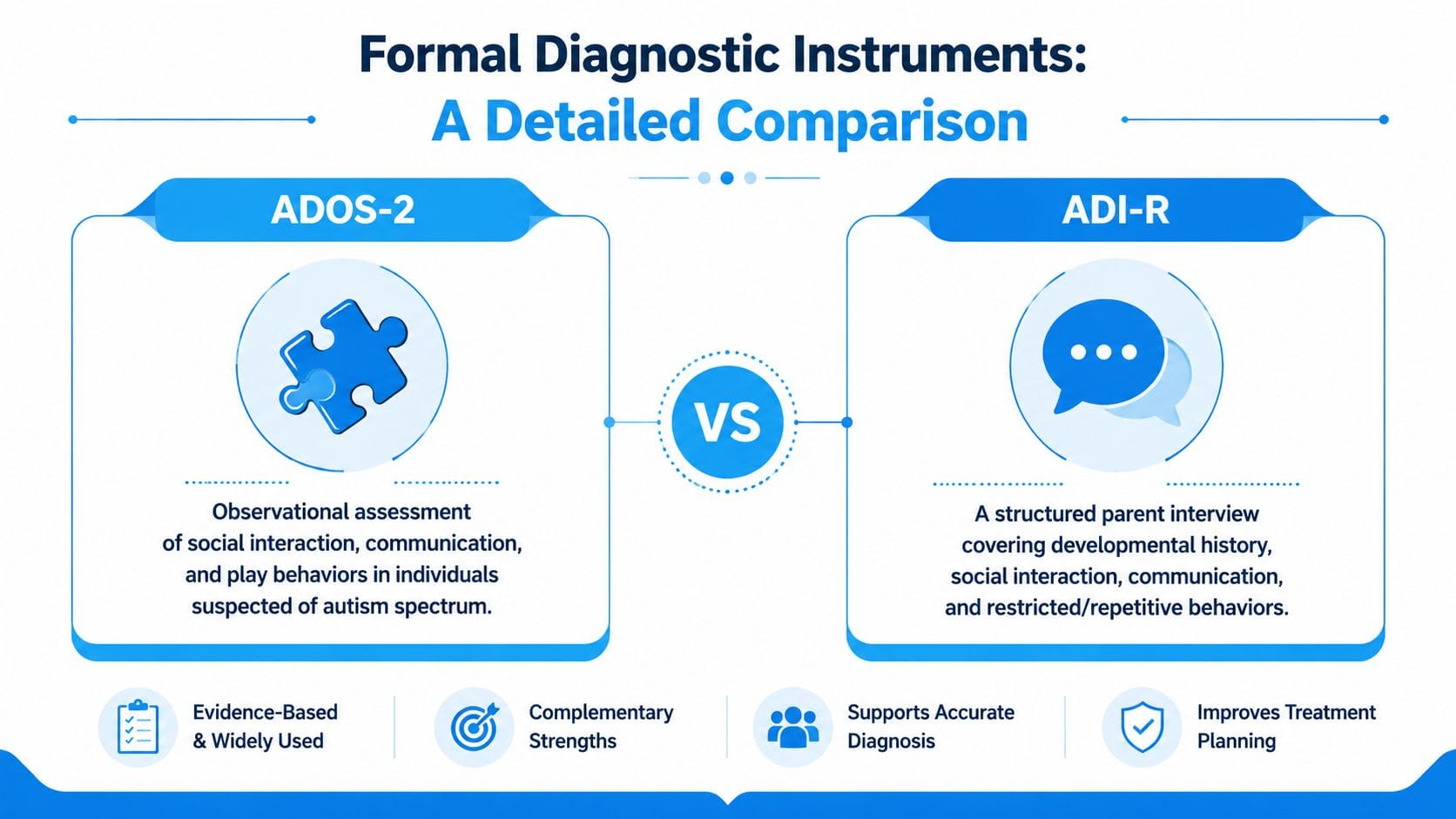
The ADOS-2 is widely treated as a key component of autism assessment. It is a structured observation, not a written quiz. The clinician watches how the child communicates, responds socially, uses play or conversation, and shows patterns of behavior that may fit autism criteria.
The ADI-R is different. It's a detailed parent interview about development and behavior over time. That long-view history matters because autism criteria must be present from early development, even if the signs looked different at younger ages.
Some evaluations may also include tools such as DISCO, RAADS-R, or AQ, depending on age and clinical context.
ADHD tools often measure a different slice of behavior
ADHD assessment usually includes interviews, rating scales, and collateral information. In some settings, a clinician may also use a performance-based tool like QbTest. According to Orange Psychological Associates' explanation of autism and ADHD assessment, QbTest is an FDA-cleared, 15 to 20 minute task that measures activity and attention to quantify ADHD-related symptoms.
That doesn't make it a diagnosis by itself. It measures behavior under test conditions. Autism instruments, by contrast, are focused much more on social communication, interaction, repetitive behavior patterns, and developmental history.
Here's a practical comparison:
| Tool Name | What It Measures | How It's Administered | Typical Age Range |
|---|---|---|---|
| M-CHAT-R | Early autism risk signals | Parent questionnaire | Toddlers 16 to 30 months |
| AQ | Autism-related traits | Self-report questionnaire | Ages 16+ |
| ADOS-2 | Social communication and behavior patterns linked to autism | Structured clinician observation | Varies by module and developmental level |
| ADI-R | Developmental history and autism-related patterns over time | Structured caregiver interview | Often used when a detailed developmental history is needed |
| QbTest | Attention, impulsivity, and activity level | Computer task with motion tracking | Ages 6 to 60 |
Some evaluations also include cognitive testing to understand learning style, reasoning, memory, and processing speed. If that comes up in your child's assessment, this plain-language guide to the Wechsler Intelligence Scale for Children can help you understand why cognitive results are often included without turning the entire evaluation into an IQ exercise.
A short overview can also help families visualize how structured autism observation works in practice.
What parents should take from all of this
The most important takeaway is that these instruments have different jobs. One observes interaction. Another gathers history. Another quantifies attention and movement. A thoughtful clinician combines those pieces instead of treating any one result as final.
If you want a parent-friendly way to recognize the core features clinicians are listening for, a DSM-5 autism checklist for parents can make the language more understandable before your appointment.
Interpreting Results and Understanding Spiky Profiles
When the report finally arrives, many parents flip straight to the diagnosis line. That's understandable. But the most useful part of the report is often the profile, not the label.
Why one child can seem both strong and struggling
A child may have strong vocabulary, solid reasoning, and a remarkable memory for favorite topics, then fall apart during worksheets, transitions, writing tasks, or multi-step instructions. Parents sometimes think this means the testing must be wrong.
Often, it means the child has a spiky profile.
A large 2024 meta-analysis of more than 1,800 neurodivergent people across 18 data sources found that autistic children and adults often performed in the typical range on verbal and nonverbal reasoning but were lower on processing speed and somewhat below average on working memory, creating that uneven pattern. In autistic children, processing speed was about 1 standard deviation below the mean according to this 2024 meta-analysis on IQ profiles in autism and ADHD.
What that looks like in daily life
A spiky profile can explain why your child:
- Sounds advanced verbally but can't finish simple classroom tasks quickly
- Understands the lesson yet misses parts of the directions
- Remembers facts in detail but loses track of materials, steps, or time
- Performs well one-on-one and struggles in busy group settings
That's why a single overall score can be misleading. Two children may have similar broad summary scores but need very different supports.
A report is most helpful when you read it like a user manual. Where does your child think well, where do they get overloaded, and what conditions help them function?
Why real life still matters after testing
Testing captures a child in a structured environment on a specific day. It doesn't always capture masking, shutdown patterns, after-school crashes, or how much effort it takes to hold it together in public.
That's one reason online self-tests and even formal measures can miss part of the picture when traits overlap. A child may appear socially capable in a short visit but struggle to sustain reciprocal interaction over time. Another may look inattentive but is mentally occupied by sensory discomfort or uncertainty in a social setting.
The best clinicians don't read scores in isolation. They ask whether the numbers fit the lived reality you and your child's teachers see every week.
Your Next Steps After an Evaluation
Once the evaluation is done, parents often feel two things at once. Relief that someone finally put words to the pattern, and uncertainty about what to do next.
A good next step isn't “fix everything.” It's to build a plan from the information you now have.
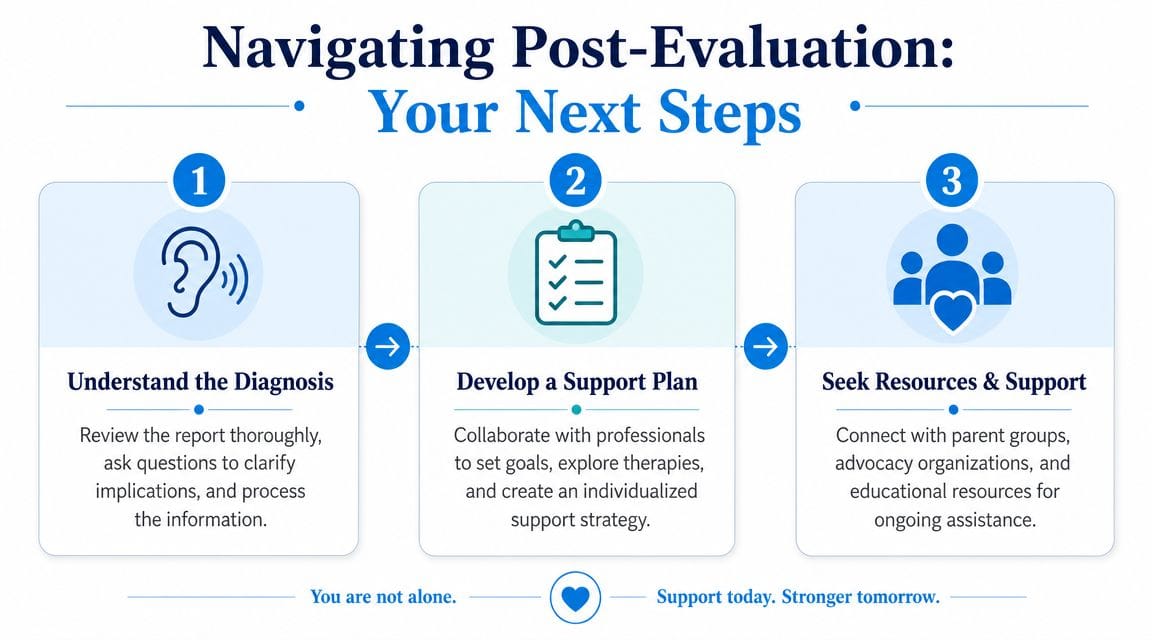
Start with the report itself
Read the full report at least twice. The first time, you may only absorb the headline. The second time, look for the descriptions of strengths, challenges, and recommendations.
Bring your questions to the follow-up conversation. Useful questions include:
- What patterns most strongly supported your conclusion
- Which concerns seem more related to attention and executive function
- Which concerns seem more related to social communication, sensory processing, or restricted patterns
- What support should start now, even if some uncertainty remains
Build support across settings
A real-world evaluation relies on more than in-clinic testing. Clinicians need longitudinal information such as early developmental history, school records, and behavior across settings because both autism and ADHD criteria depend on symptoms being present from childhood and in different environments, as explained in this overview of autism and ADHD testing inputs.
That same principle should guide what happens next. Support usually works best when home, school, and outside providers are all looking at the same child, not three different versions of the story.
A practical checklist for families
Schedule the follow-up
Don't leave with unanswered questions if the report language is dense or technical.Share the right documents with school
Ask what the school needs to consider accommodations, supports, or formal educational planning.Organize therapy recommendations
Some children may need occupational therapy, speech-language support, behavioral consultation, parent coaching, or a medication conversation. The report should help prioritize.Track what happens after changes begin
Once school accommodations, routines, or therapies start, keep notes on what improves and what still gets stuck.Watch function, not just symptoms
The central question is not whether your child still “looks autistic” or “looks ADHD.” It's whether daily life is becoming easier, safer, and more sustainable.
Bring examples to every follow-up visit. “He struggles with transitions” is less useful than “He has the hardest time moving from preferred activities to homework, especially on short-sleep days.”
Parents often feel pressure to understand every recommendation immediately. You don't need to do that. Start with the supports that reduce stress in the most important parts of your child's day.
Prepare for an Assessment with Guiding Growth
The most valuable thing you can bring to an autism adhd test process isn't a perfect theory. It's organized, real-world information.
Clinicians need patterns. They need to know what happened, when it happened, what came before it, how long it lasted, how your child recovered, and whether the same thing happens at home, school, bedtime, or during transitions. That's hard to reconstruct from memory or scattered notes.
A structured tracker can help parents log meltdowns, shutdowns, sleep changes, sensory triggers, routines, appointments, and questions for providers in one place. One example is Guiding Growth, which is designed to help families record behavior, sleep, nutrition, medications, and therapy information, then share organized reports with caregivers or clinicians. If you're getting ready for an evaluation, this guide on how to organize autism records for evaluations is a useful place to start.
That kind of preparation doesn't replace clinical judgment. It gives the clinician better evidence to work with, and it helps you walk into the appointment feeling clearer, calmer, and more confident.
If you want a simpler way to track behaviors, routines, sleep, appointments, and the patterns clinicians ask about, Guiding Growth can help you turn everyday observations into organized records you can use at evaluations, school meetings, and follow-up care.
Crafted with Outrank


